The SRC investements in VHVs education and thus in the promotion of primary health care services
Front line health promoter in the remote villages of Lao PDR
De Binita Poudel et
Joan Carlo Mayangitan
Even though effectively engaging Village Health Volunteers (VHVs) and managing the VHV system have been proven to be two of the most cost-efficient strategies in improving health indicators of the country, challenges to financially sustain, scaling up, and scaling out the scope of their work prevail. VHVs play a crucial role to facilitate referral pathways to health facilities and provide first-hand information to the most vulnerable groups. However, the supervision and monitoring of those interventions haven’t yet been streamlined in the Lao context.
Lao People’s Democratic Republic (Lao PDR) is a low-middle income country in Southeast Asia with a total population of 7.2 million (2020). In rural areas, access to quality health care services is at minimal. Aside from infrastructural and socioeconomic barriers, shortage of trained human resources is one of the most important factors which hinders the service provision of quality health care services.
Based on Lao PDR National Health Statistics 2019, the average number of skilled health workers per 1000 population was 2.40 which meets the World Health Organization requirement on the ratio of 2.30.
In Lao PDR, VHVs are responsible for education on most of the primary care services to the communities. VHVs are primarily unpaid lay workers mostly used by national programs and other external service delivery projects. VHVs have officially been a part of the Lao PDR health system since 2000 when Government released its ‘Policy on Primary Health Care’ as part of the model healthy village strategy.
VHVs are primarily unpaid lay workers mostly used by national programs and other external service delivery projects.
VHVs role still not clearly defined despite its integral part of the health system
Even though VHVs have been recognized to be an integral part of the health system. Ministry of Health had a training program for VHVs for six months with the support from Asian Development Bank with the aspiration to formalize VHV’s work into the public civil servant function. However, it has not been fully implemented throughout the country and VHV’s role is not clearly defined in the overall health structure at the health center level. Likewise, the role of health center staff towards monitoring VHVs and reporting about the VHVs work is not clear.
Further challenges arise when VHVs migrate due to various reasons. Recruiting new VHVs and training them on various health issues requires a huge amount of time and resources. Many international partners and NGOs have been actively engaged in direct service delivery initiatives in selected districts and provinces of Lao PDR. Most of these initiatives use VHVs as a mechanism to address the shortage of professional healthcare staff to operate at community level.
The Swiss Red Cross (SRC) has been supporting VHVs to build their capacity to increase demand at health centers and promote access to health services in collaboration with the Provincial Health Department in Chomphet and Phonexay districts of Luang Prabang since 2013. The Maternal and Neonatal and Child Health Project targeted both district hospitals and 10 out of 17 health centers with an intervention package aiming at putting the National policy on reproductive, maternal, neonatal and child health into practice. In these target districts, there has been a positive impact on maternal, neonatal and child health healthcare seeking behavior. This was achieved through combined SRC health center preparedness support, outreach and referral logistic support and health promotion activities by Health Centre staff, as well as by mobilizing the “community system” through VHVs and Village Health Committees.
Many international partners and NGOs have been actively engaged in direct service delivery initiatives in selected districts and provinces of Lao PDR. Most of these initiatives use VHVs as a mechanism to address the shortage of professional healthcare staff to operate at community level.
The community system consists of 262 VHVs distributed in 131 villages in the two districts. In both districts, each village has a maximum of 2 VHVs and the population for each village ranges between 150 and 1,700 people. Currently, VHVs are often selected by the village head, which are mostly men.
VHVs doeducation on maternal and child health in the village with a focus on behavior change and linking people to health services. They follow up care to mothers and babies, assist health center staff in outreach and immunization, assist with deliveries of babies,andassist in homes visits. They conduct regular monthly growth monitoring of children aged less than five years, provide an opportunity to give tailored nutrition education and ensure referral of serious cases. The performance of the VHVs also varies due to their gender roles when it comes to their specific duties. Sometimes the issues around the maternal and neonatal health are better advocated by the female VHVs than male VHVs.
The SRC invests in the community health care system with various measures
To address the shortage of professional primary care health workers SRC invested heavily in training and equipping VHVs. A series of workshops had been offered to the VHV to build their capacity, this includes nutrition and breastfeeding, communication and counseling, malnutrition and growth monitoring. Meetings and supervisions were also conducted at regular interval to keep the VHVs active in their villages. In Chompet and Phonexay, VHVs received 4 days of initial training and follow up training every year. SRC also provided growth monitoring equipment (weighing scales and height measuring boards) to VHVs as well as hats, bags and t-shirts.
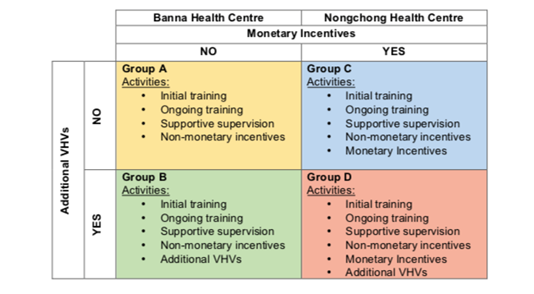
In 2018, the SRC, Provincial health Department and the District Health Offices conducted a VHV pilot intervention to determine whether changes to the current Lao VHV system can be achieved through various activities, to see if more active and motivated VHVs can occur, and to determine if these changes will result in improved population health outcomes. The study took place at catchment areas of two Health Centers (Banna and NongChong) in Chompet district. VHVs from 2 Health Centers catchment areas were divided into 4 intervention groups and applied different treatments to determine the effect.
The community system consists of 262 VHVs distributed in 131 villages in the two districts. In both districts, each village has a maximum of 2 VHVs and the population for each village ranges between 150 and 1,700 people.
A VHV pilot intervention to determine whether changes to the current Lao VHV system can be achieved through various activities, to see if more active and motivated VHVs can occur, and to determine if these changes will result in improved population health outcomes.
The evaluation of the VHV pilot intervention showed the existing challenges
The evaluation of the VHV pilot intervention employed qualitative and quantitative data collection methods, which include desk review, focus group discussions, in-dept interviews, review and collection of monitoring reports. The objective of the evaluation was to determine the successes and challenges of the project, and how to move forward with the lessons learned. Five major themes were emerged from the qualitative data analysis. These included: the role of VHVs, ethnic groups, reporting VHV data, monetary incentives and village profiles including community dynamics and respect.
Based on the findings the improvements were seen to all VHVs in all catchment areas in regard to conducting health education; counselling at homes; and outreach days as they shared the knowledge either informally with family and friends, or formally at a village meeting after the training. In Lao PDR there are three main ethnic groups: Lao lum, Homong, Khmu. The challenges for VHVs working in Hmong villages was found across all catchment areas. When Lao or Khmu VHVs and heads of village discuss Hmong populations, they frequently expressed that Hmong families do not respect or choose health care, but instead, they prefer the use of traditional trees when their children have problems, they know about the healthcare but they are not interested. Khmu and Lao VHVs also expressed challenges in family dynamics within the Hmong population, with the male-centred household often difficult to convince regarding delivery at health centres and immunisation.
Table 1. VHV Pilot intervention groups
When Lao or Khmu VHVs and heads of village discuss Hmong populations, they frequently expressed that Hmong families do not respect or choose health care, but instead, they prefer the use of traditional trees when their children have problems, they know about the healthcare but they are not interested.
During the quantitative investigation, the lack of consistent reporting was seen across all intervention groups due to lack of clarity in regards to dates to be sent and lack of blank forms. In regards to monetary incentives, the challenges seen during the pilot intervention were some VHVs believed they were owed payment for referrals, and the delay in time between payments created confusion. The cross-checking of data for payment was also challenging, with reported referrals often not found in the health centre books, or patients taking themselves straight to the district or provincial hospitals. Most VHVs reported feeling motivated and well respected by their communities, with very few feeling as though their voices were not heard. Heads of village also spoke highly of the VHVs, respecting their roles and often inviting them to speak at village meetings.
Guidelines of VHV roles and responsibilities should be disseminated, so all are clear of the expectations and health centers should have a supply of reporting forms.
Recommendations for future government projects engaging VHVs would be
that there should only be two VHVs per village as adding more VHVs does
not reduce workload but instead adds a burden to the health workers to
liaise with many people and also duplicate reporting become common. In
Hmong villages, one VHV should be male, as the men are often more
respected by husbands of the community. Regarding monetary incentives, a
system can be created with easy follow up and a simple payment method,
Furthermore, guidelines of VHV roles and responsibilities should be
disseminated, so all are clear of the expectations and health centers
should have a supply of reporting forms.
References:
Lao Statistics Bureau (2020). Laos Demographics Profile 2020
Lao Statistics Bureau (2012). Laos Demographics Profile 2012
Binita Poudel, Head of Sub-Delegation is
working in Lao PDR at Swiss Red Cross. Binita has worked and managed public health
projects in Nepal, Bangladesh, South Sudan in the different Red Cross and Red
Cresent societies. Email
Joan Carlo Mayangitan, RN, MAN, MSc is
working for Swiss Red Cross in Lao PDR for four years focusing on Monitoring
and Evaluation and Disaster Risk Management. Email