How the application of Systems Thinking tools supported district health managers adapt to the emerging challenges of the COVID-19 crisis
Systems Thinking approaches for more resilient health systems during COVID-19
By Carmen Sant Fruchtman,
Shamsa Zafar,
Daniel Cobos,
Muhammad Bilal and
Helen Prytherch
The COVID-19 pandemic has revealed the majority of health systems were not prepared for the magnitude of such a shock. Behind this were weaknesses that had been long covered in the system. In this article, we compile the lessons learned of applying systems thinking during the pandemic and argue that to achieve more resilient health systems, systems thinking should become part of the routine practice of decision-makers, implementers and researchers.
Reading time 4 min
Practical Systems Thinking Tools developed within ST-DHS. Photo: @ Child Advocacy International
Funded by the Alliance for Health Policy and
Systems Research (AHPSR), the Swiss Tropical and Public Health Institute (Swiss
TPH) hosts a Technical Support Centre (TSC) with expertise in health systems
resilience and district-level health systems strengthening. The Centre has been
facilitating the adaptation of systems thinking tools, and exchanging about how
to achieve system-wide change with district health management teams in
Botswana, Pakistan and Timor-Leste since the onset of the pandemic. Swiss TPH
works together with institutions in each country to achieve this endeavor: the
Institute for Development Management in Botswana, Child Advocacy International
in Pakistan and the World Health Organization for the country office in
Timor-Leste.
The Systems Thinking for District Health
Systems initiative was launched in November 2019. The original approach
included mostly the work of each national institution together with the TSC at
Swiss TPH to adapt and apply systems thinking tools to the needs of district
health managers. The TSC was going to facilitate the adaptation, capacity
building and monitoring of the initiative.
How the pandemic forced us into new forms of cooperation and exchange
In March 2020, driven by the ongoing challenges of the COVID-19 pandemic, we had to rethink how we would operationalize the initiative, as face-to-face implementation became impossible. This shift led to the creation of an online District Systems Thinking Community of Practice (CoP). The CoP emerged as a way to conduct capacity-building activities and establish a structure to learn from each other.The CoP sessions became a place for exchange and discussion, instead of vertical capacity building, which indirectly led to a more equal partnership, with multidirectional learning.
Before the pandemic began, the TSC had organised a 3-day preparatory workshop with the institutions in which the main concepts of systems thinking were introduced and some practical examples of the use of systems thinking tools (decision space, reflective practice and embedded research) were given. The workshop aimed to provide practical skills to participants in the use of systems thinking approaches and tools and provided a basis for the whole initiative.
Moreover, from the very
outset, the TSC aimed to facilitate peer-to-peer learning and build on the
countries expertise. The participants were initially invited quite informally
to engage and share their experiences in terms of system thinking, and how to
respond to the pandemic, in an attempt to promote learning across countries.
The Community of
Practice (CoP) was formally launched in June 2020. After the initial
technical discussions around approaches and tools, the CoP consolidated its
focus on the exchange of experiences across countries. It was
also through the use of this platform that brainstorming occurred around how to
engage with, and support, district teams within the COVID-19 context. The country
institutions discussed their progress and challenges to jointly find solutions
for these challenges, noting that some travel within a country context was
possible at various points in the timeframe of the pandemic (Figure 2).
CoP reflective practice session (December 2020). Photo: @ Swiss TPH
The institutions in each country managed to
build and establish new relationships with district health managers. District
stakeholders were involved in the CoP in an indirect way via the national institutions,
and when their agendas and connectivity allowed, they also joined to see how
the systems thinking resources and material could provide support.
Illustratively, in Pakistan, the identified health system challenge was the
strengthening of the COVID-19 contact tracing strategy in Islamabad (see also
the case study below, while in Rajanpur, Pakistan, Botswana and Timor-Leste it
was the coordination mechanisms at the district level and the strengthening of
the district health information system).
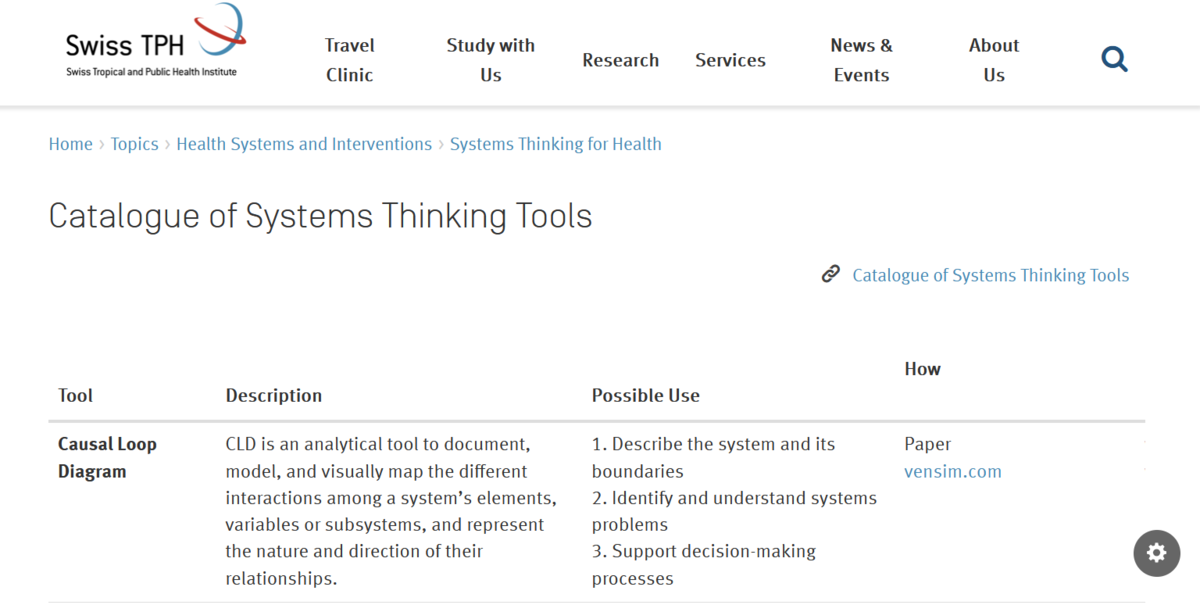
A repository of the systems thinking tools is now publically available, with their application shown in Figure 3 below, and all accessed here: Systems Thinking Tools (swisstph.ch)
Figure 3: Systems Thinking Tool Catalogue
Case study from Islamabad Capital Territory (ICT)
The research team at Child Advocacy International (CAI) engaged with the district health management team (DHMT) in Islamabad at the end of the first quarter of 2020 and established a routine relationship. Both these teams worked together and identified COVID-19 contact tracingstrategy in ICT as the health system component to be addressed by applying systems thinking. For this, the CAI team facilitated reflective practice sessions with the DHMT, to understand the process and structure behind the contact tracing system, as well as the main drivers of the challenges faced. The district team together with CAI and the TSC went on to develop a process map illustrating the different stakeholders and steps in the contact tracing system of Islamabad and identified the main bottleneck to address.
This allowed highlighting and reinforcing the existing success factors behind the contact tracing system, such as:
Establishment of National and District Surveillance hubs of coordination and information,
Introduction of active rather than passive surveillance; and
Prompt scale up of service and resource mobilization.
The discussion and visualization of the process map triggered action to address some pain points, such as:
Delay in the COVID-19 patient information flow, from the testing points to surveillance activities;
Distal surveillance information pathways, such as those in the rural parts of the city; and
Capping of the daily contacts traced owing to missing information.
This work resulted in strengthening the information system and contact tracing approach, based on a holistic view of the operationalization and evolution of ICT activities.
Reflective practice session with Islamabad's DHMT. Photo: @ Child Advocacy International
The learnings of this process are currently being reported in a peer-reviewed publication. Furthermore, a video explaining the approach take and the learnings from applying process mapping, can be accessed here.
Resilient health systems require a Systems Thinking approach
Health systems around the world were caught unprepared for the COVID-19 pandemic. In particular, these systems were revealed to operate in under-financed, siloed sub-systems. As a result, they lacked the resilience to adapt to the emerging crisis, and even the tools to understand the situation in time. The existing silos challenged timely coordination and communication between key stakeholders, including communities. They laid bare inefficiencies, brought many services to a halt, and overwhelmed health workers trying to respond to very high numbers of acute cases without the necessary protection or resources.
Ideally, health systems should be able to absorb and adapt to external shocks and emergencies to maintain essential services, while also generating and using data to inform decisions and make changes. Resilience has been described as “the capacity of a system to absorb disturbance and reorganize while undergoing change to still retain essentially the same function, structure, identity, and feedback”. (Walker, B. et al. 2004)
Ideally, health systems should be able to absorb and adapt to external shocks and emergencies to maintain essential services, while also generating and using data to inform decisions and make changes.
In our experience, achieving resilient health systems is tightly linked
with the application of systems thinking approaches. The learnings from
the ST-DHS initiative during the COVID-19 pandemic highlight that even
in resource-poor settings, systems thinking tools and approaches can be
beneficial for district health systems. Applying a systems thinking lens
can help health system managers gain an overview of the source of
problems, be more confident in proposing solutions, while also
monitoring and reflecting on the changes, and being able to
course-correct as and whenneeded.
Reference
Walker, B., C. S. Holling, S. R. Carpenter, and A. Kinzig. 2004.
Resilience, adaptability and transformability in social–ecological
systems. Ecology and Society 9(2): 5. [online] URL: http://www.ecologyandsociety.org/vol9/iss2/art5/
Carmen Sant Fruchtman is a scientific collaborator at the Swiss Tropical and Public Health Institute, Basel, Switzerland. She holds a Master of International Health from the same institution, where she has been working for over 5 years. Her research interests include the adaptation of systems thinking tools for practical use, as well as redesigning health systems to leave no one behind. Email
Professor Shamsa Zafar is an obstetrician at Fazaia Medical College with over 15 years of experience in public health. She holds a PhD from University of Liverpool in maternal psychosocial health.
Dr. Daniel Cobosis a physician and a health system researcher affiliated with the Swiss Tropical and Public Health Institute with a focus on the application of systems thinking tools and methods to unpack the inherent complexity of public health challenges. He leads the “Systems thinking for district health systems (ST-DHS)” project funded by AHPSR and the capacity-building workstream within the Systems Thinking Accelerator (SYSTAC). As a member of the WHO Reference Group on Health Statistics (WHO RGHS),he has led the systems analysis of civil registration and vital statistics (CRVS) in more than 25 countries across Africa, Asia, and Latin America using discrete event modeling.
Dr. Muhammad Bilal is a public health practitioner with expertise in qualitative research methods in health systems research. His interests lie in health systems and the use of systems thinking for healthcare in LMICs.
Helen Prytherch is a Public Health Specialist and Head of Unit at the Swiss Centre for International Health. By training a registered nurse and qualitative social scientist, she has 17 years’ work experience gained at all levels of the health system across a variety of countries in Asia, Latin America and sub-Saharan Africa. Helen is besides this a board member of the Network Medicus Mundi Switzerland.
The need for health system strengthening - a key insight in the pandemic