An appeal by Nadya Wells, Senior Research Adviser at the Geneva Graduate Institute (IHEID)
Combatting the ‘Silent Pandemic’ of Antimicrobial Resistance: Break out the Pots and Pans Again
By Nadya Wells
Fleming’s revolutionary discovery of penicillin in 1928, allowed modern medicine to flourish. New classes of antibiotics emerged until the 1980s, but Fleming warned antibiotic usage inevitably leads to bacteria developing resistance. Fast forward, indeed some are now resistant to the majority of today’s antibiotic arsenal, a crisis World Health Organization (WHO) puts in the top 10 public health threats facing humanity. A Lancet study found 1.27 million deaths in 2019 attributable to antimicrobial resistance (AMR), and 4.95 million AMR associated deaths (Murray CJ. et al., 2022). Containment requires international and multisectoral co-operation, a hard global health governance task.
Reading time 4 min
Foto von Clem Onojeghuo auf Unsplash
WHO Global Research Agenda: A Recipe Book for Action
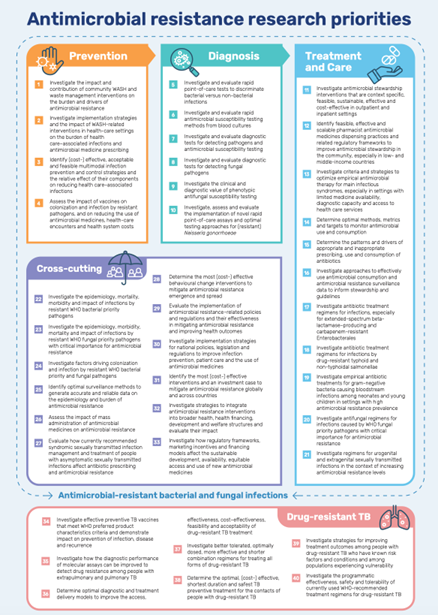
In June 2023, WHO published a global research agenda (WHO, 2023): forty priorities, in eleven areas, across five themes. Essentially a recipe book to galvanise concrete research proposals, fundable by donors, implementable across economic contexts, concentrated on WHO priority pathogens. It aims to guide policy-makers, researchers, funders, implementers, industry and civil society in evidence generation for collective efforts to contain AMR in humans. From analysis of a decade of 3000 published documents, experts prioritised 2000 knowledge gaps, developing 40 critical research topics, answering concerns that without prioritisation, the multitude of possible interventions risked paralysing action (Wellcome, 2020).
WHO (2023): Global research agenda for antimicrobial resistance in human health, Policy Brief
So will it work? The past demonstrates the first major challenge will be funding. In 2015, WHO published a ‘One Health’ framework to tackle AMR, bringing together human and veterinary medicine, and agricultural and environmental sectors to which G7, G20 and other countries committed. In September 2023, the Organisation for Economic Co-operation and Development (OECD) produced a policy brief on ‘Embracing a One Health Framework to Fight Antimicrobial Resistance’ (OECD, 2023). They found unfunded national AMR programmes, “a fraction of them incorporated financial provisions to implement their plans”. Convincing policy makers to fund tackling a slow-moving invisible threat is notoriously challenging, parallels with climate change are clear.
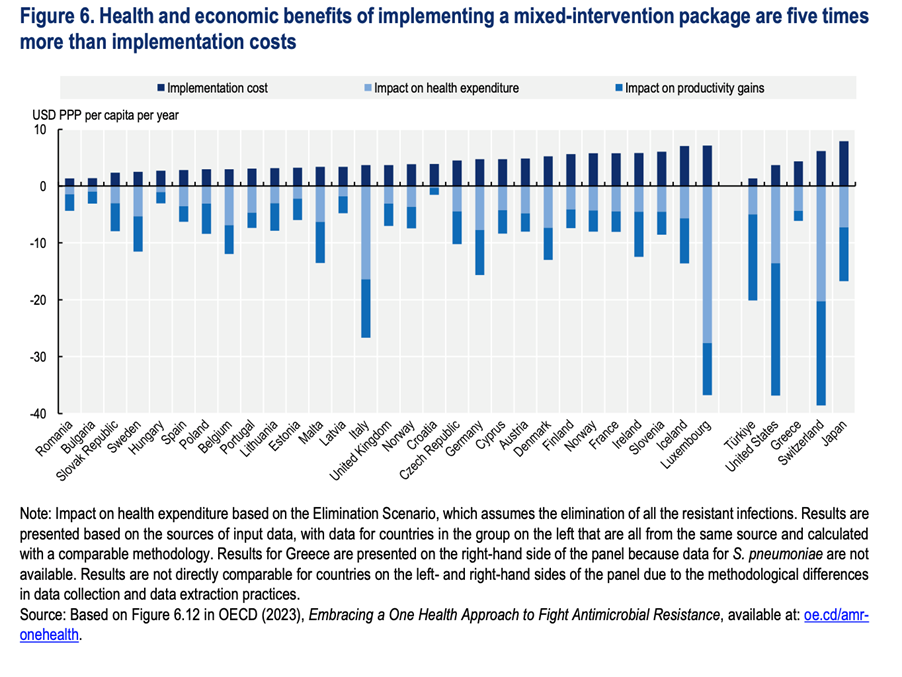
This is an essential barrier to overcome, requiring long-term funding structures with governance independent of short-term domestic politics. To convince holders of the purse strings, OECD produced an evidence base, demonstrating macroeconomic costs of inaction, and impact on the labour force. They outline affordability of hospital, community and mixed policy packages, showing they will pay for themselves. Seven of eleven modelled interventions cost less than $1 per capita per year, with a return on investment of 2.3-24.6x. Switzerland could be a major beneficiary of savings in healthcare costs and improved productivity.
OECD found unfunded national AMR programmes, “a fraction of them incorporated financial provisions to implement their plans”.
OECD (2023): Embracing a One Health Framework to Fight Antimicrobial Resistance
Source: OECD 2023, Embracing a One Health Approach to Fight Antimicrobial Resistance. https://doi.org/10.1787/ce44c755-en
What role for Switzerland?
Governments, especially in high-income countries, now need to provide the missing ingredients; Switzerland has much to offer. As an early adopter of ‘One Health’ approaches at home, expertise can be shared in twinning exercises with countries starting implementation. On infection prevention and control and hand hygiene Switzerland has world leading technical expertise and a WHO collaborating centre at the Geneva University Hospital, with national surveillance experience at ANRESIS and Swissnoso.
In Basel, a developed ecosystem including academia, startups, policy makers and innovation agencies running multi-disciplinary research programmes aligns with the WHO agenda. Swiss biopharmaceutical companies continue to research treatment and diagnostics, and have been joined in Basel by the AMR Action Fund, a $1bn public private partnership to support development of novel antibiotics.
Switzerland has much to offer. As an early adopter of ‘One Health’ approaches at home, expertise can be shared in twinning exercises with countries starting implementation.
Invisible Threat: The So-Called ‘Silent Pandemic’
However, the second major challenge is invisibility. With lives and the global economy at risk, why is this major global health threat often referred to as the ‘Silent Pandemic’ (Rayan RA, 2023)? Besides not funding enough, we have not convinced political leaders, or the public, of the urgency. The AMR pandemic is unlike Covid-19 where in our daily lives we saw masks and prevention posters in streets worldwide. To the general public, the human consequences of AMR are hidden. Deaths, not from a named disease, but dying when treatments fail. A lack of adequate diagnostics keeps resistant infections uncounted. Naming the pandemic ‘silent’ almost gives it an excuse to remain hidden.
Besides not funding enough, we have not convinced political leaders, or the public, of the urgency.
Pexels Photo by Rosemary Ketchum: https://www.pexels.com/de-de/foto/menschen-die-sich-auf-der-strasse-versammeln-1464223/
Stop the Silence: Start Banging the Pandemic Pots and Pans Again
Both WHO and OECD packages outline the need for better public communication. To galvanise attention, increase visibility and unlock funding, maybe we need the public to consider loudly banging cooking pots again, globally, as we did during the Covid-19 pandemic, this time in support of healthcare workers on the AMR frontline.The new research agenda is a ‘Call to Action’ with tailored recommendations considering the higher burden and different needs of AMR response in low-resource health systems. In the last three months WHO provided the recipe book, OECD provided the cost-benefit analysis. Ideally the healthcare cost savings and benefits of productivity will be applied to funding the research agenda. Funding and visibility, critical ingredients to make the response deliver this time.
To galvanise attention, increase visibility and unlock funding, maybe we need the public to consider loudly banging cooking pots again, globally, as we did during the Covid-19 pandemic, this time in support of healthcare workers on the AMR frontline.
The Global Health Centre (GHC) is one of the research centres of the Geneva Graduate Institute focusing on global health governance.
References
Murray CJ, Ikuta KS, Sharara F, Swetschinski L, Robles Aguilar G, Gray A, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. The Lancet. 2022 Feb;399(10325):629–55.
OECD. Embracing a One Health Framework to Fight Antimicrobial Resistance
[Internet]. OECD; 2023 [cited 2023 Sep 25]. (OECD Health Policy
Studies). Available from: https://www.oecd-ilibrary.org/docserver/ce44c755-e...
Nadya Wells, Senior Research Adviser, Global Health Centre, Geneva Graduate Institute. Nadya is an experienced investment professional whose passion is building bridges to facilitate increased financing for global health. She is currently working on the FINPHARM project, funded by the Swiss National Science Foundation, exploring the impact of Financialisation on Global Health through a series of pharmaceutical case studies where she is leading the work on anti-microbial resistance (AMR). Email