How the set up of a task force has catalyst the implementation of safe abortion care (SAC)
Safe Abortion Care: What Practice is Being Followed by MSF?
Von Nelly Staderini
For some years now, Médecins sans Frontières (MSF) has been investing in safe abortion care. In 2004, MSF drew up an institutional statement on abortion care. In 2014, the organisation undertook a critical internal review which revealed the slow progress that was being made to integrate abortion care into healthcare practices. This review analysed the barriers existing for people who were seeking or receiving care. A dedicated task force was set up with the intention to swiftly increase access to safe abortion care. Now, a few years after innovative tools have been used to implement this dedicated strategy, the results are available and can be shared with a broader external audience. In the past three years, MSF was able to provide more than 35,000 safe abortions annually. However, despite this success, the availability of safe abortion care remains precarious in many settings.
A recent WHO report (The Lancet, 2023) reveals that, between 2016 and 2020, there was no improvement or even a deterioration in the maternal mortality rate in most regions of the world. A total of 287,000 maternal deaths were reported worldwide in 2020 and over 13% of these deaths were attributed to unsafe abortions. This is a recognised leading cause of mortality but also one which is entirely preventable by the implementation of safe abortion care. A total of 45% of all abortions are unsafe; 97% of these are carried out in developing countries.
Key drivers behind the lack of provision of safe abortion care are the highly politicised nature of the issue and the fact that it is influenced by personal beliefs and attitudes.
Key drivers behind the lack of provision of safe abortion care are the highly politicised nature of the issue and the fact that it is influenced by personal beliefs and attitudes.
What measures did we take?
In 2015, the MSF working group on sexual and reproductive health proposed the innovative strategic model of setting up a task force to support the implementation ofsafe abortion care in relevant projects.
This task force was endorsed and supported internally at the organisation’s highest level and MSF made it clear that it was an operational priority to instigate the change. The rationale behind the task force was for it to work as a catalyst in the creation of dedicated human resources that could create a safe environment to open dialogue, pilot initiatives and disseminate tools to help teams in the field implement the safe abortion policy.
Since then, various models of care have been piloted, including self-medicated abortion. Sensitisation work, training and research have been carried out to increase knowledge and understanding within MSF about the requirements and medical solutions. Today, medicated abortion is generally undertaken with a low complication rate and is not usually associated with mortality.
This task force was endorsed and supported internally at the organisation’s highest level and MSF made it clear that it was an operational priority to instigate the change.
How does this translate into care provision?
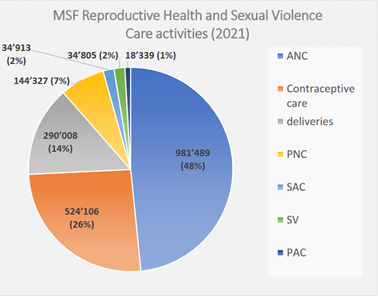
Every year, MSF as a whole provides around a million antenatal consultations and half a million appointments for contraceptive care as well as delivering nearly 300,000 infants. This constitutes the majority of the organisation’s sexual and reproductive health activities. In addition, in the past three years MSF provided more than 35,000 instances of safe abortion care annually (cf. Fig 1 for 2021). Today, medicated abortion with misoprostol is chiefly carried out with a low rate of complications and zero associated mortality.
Fig 1
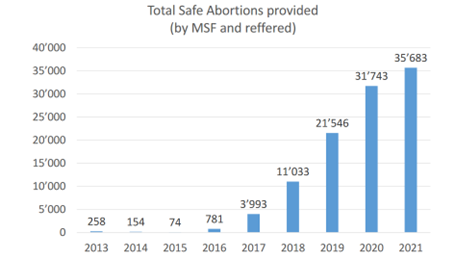
It is important to note the growing trend in the provision of safe abortion care in the past few years. This demonstrates what a success the task force initiative has been (cf. Fig 2).
Fig 2
The primary objective of the tools designed by the task force has been to help teams working in the field to move from a climate of fear to one that enables safe abortion care to be provided.
One of these tools has been the adaptation of the VCAT from the Ipas (IPAS, 2018) to MSF stakeholders to create a safe space in which to reflect on the values and attitudes held by MSF staff. This one-day workshop was piloted at the organisation’s Geneva Headquarters in 2016 and was then rolled out at a regional and country level. Today, the workshops have become a routine activity which is undertaken on a monthly basis due to the high turnover of staff at MSF and the variety of backgrounds from which these staff derive.
Further tools such as a list of steps for implementation, algorithms, training materials (How to use abortion pills) including for self-medication and internal training videos have all been developed and continue to be shared within MSF to ensure a continuity in the provision of care. These materials have been translated into many languages to enable staff from any country to access the same information. This translation work has been recognised as a key strategy to disseminate the use of these tools to support their implementation.
However, there is still a lot of work to be done. Despite the investment of dedicated staff to support teams in the field, missed opportunities still occur every day in challenging contexts. Pilot projects are required to provide a more innovative model of care which allows for a patient-centred approach and gives increased access to the self-medicated option which can be very effective in many contexts and is the preferred choice for many women due to its confidential nature. We should also dedicate more time within the organisation to sharing experiences so we can enable staff to learn from each other. In addition, a number of publications (Schulte-Hillen, C. et al., 2016; Kumar, M. et al., 2022; Kumar, M et al., 2020) and some communication work (MSF, 2021a; MSF, 2021b; MSF, 2022a; MSF, 2022b; MSF 2023) aimed at external audiences has allowed MSF to share the results of the work undertaken.
This one-day workshop was piloted at the organisation’s Geneva Headquarters in 2016 and was then rolled out at a regional and country level. Today, the workshops have become a routine activity which is undertaken on a monthly basis due to the high turnover of staff at MSF and the variety of backgrounds from which these staff derive.
The patient-based approach as a key strategic pillar of MSF intervention is a paradigm shift that is helping to empower women to make decisions about their own health. This approach requires recognition and support as an innovative strategy which yields excellent results.
The work undertaken in recent years by MSF on safe abortion care can be recognised as a historic success. It has affected the organisation as a whole with questions related to MSF’s identity, ambitions and positioning and has contributed to change.
This work has also enabled MSF to share lessons learnedwith external partners at bilateral meetings and conferences and to communicate about the care provided by the organisation and the manner of and reasons for this provision.
However, sustainable change demands continuous engagement, beginning with the human resources who require information on safe abortion care to be better prepared to meet the needs of their patients. This must start with the recruitment of staff and continue into their training andretention.
Challenges and the way forward
Today in MSF, the goal is to shift safe abortion care from being a catalyst in the hands of the few driving the process into one of sustained ownership with a broader leadership, integrating it into the handsof the many.
This is the only strategical step which will ensure that safe abortion care is integrated into routine MSF medicalwork. A major evolution has been achieved but the policy currently remains fragile because stigma, legal frameworks, and the politicisation and polarisation of abortion remain as external barriers. A high staff turnover at MSF coupled with fearfulness and a lack of prioritisation are additional internal barriers that require permanent attention.
And, given the sensitivity and political nature ofabortion, MSF must invest in its capacity to respond to both challenges and opportunities as theyarise.
In conclusion, the lack of access to safe, timely, affordable and respectful abortion care is a critical public health and human rights issue that demands to be addressed.
A major evolution has been achieved but the policy currently remains fragile because stigma, legal frameworks, and the politicisation and polarisation of abortion remain as external barriers.
Kumar M, Daly M, De Plecker E, et al, Now is the time: a call for increased access to contraception and safe abortion care during the COVID-19 pandemic. BMJ Global Health (2020);5:e003175. https://gh.bmj.com/content/5/7/e003175
Kumar M, Schulte-Hillen C, De Plecker E, Van Haver A, Marques SG, Daly M, Vochten H, Merzaghi L, de le Vingne B, Saint-Sauveur JF. Catalyst for change: Lessons learned from overcoming barriers to providing safe abortion care in Médecins Sans Frontières projects. Perspect Sex Reprod Health. (2022 Oct 23). doi: 10.1363/psrh.12209. Epub ahead of print. PMID: 36273433. https://pubmed.ncbi.nlm.nih.gov/36273433/
Schulte-Hillen, C., Staderini, N. & Saint-Sauveur, JF. Why Médecins Sans Frontières (MSF) provides safe abortion care and what that involves. Confl Health 10, 19 (2016). https://doi.org/10.1186/s13031-016-0086-5
Nelly Staderini is a French Midwife with Public Health diploma in community approaches. She has extensive field experience in various Humanitarian contexts including Pakistan, Afghanistan, Chad and Burundi. For more than 12 years, she has been working in the Medical Department of Médecins Sans Frontières (MSF) Headquarters in Geneva as the Sexual, Reproductive Health and Sexual Violence Advisor. Since 2019 she is the Medical leader of the Women and Children’s Health Unit. She has worked in recent years on abortion, its better integration as essential health care, the simplification of its model of care and the women’s autonomy. She is the author of various publications including a photo book on Afghan women. E-Mail