Swiss Agency for Development and Cooperation (SDC) Healthy Life Project Moldova
Using integrated care modalities to address social determinants of health and inequalities in rural Moldova
Von Tatiana Dnestrean,
Ala Curteanu,
Octavian Pascaru und
Helen Prytherch
The Republic of Moldova is affected by demographic changes with high outbound migration of the working population in search of better economic opportunity (73.7%), and a remaining ageing population (ageing coefficient 23,8 in 2022). Moreover, the country faces a high burden of Noncommunicable diseases (NCDs). NCDs account for more than 80% of all deaths in the Republic of Moldova. In addition, circulatory system diseases (CVDs), cancers, diabetes and respiratory diseases are responsible for about four out of 10 cases of primary disability [STEPS 2021].
Moldova remains a mainly rural country where central and local governments struggle to ensure service provision. Much of the older population is at risk of, or has developed, one or multiple NCDs. In 2021, about 31.1% of the total population indicated that they suffer from at least one NCD, and 47.3% indicated that they suffer from at least two. Moreover, the elderly are most likely to reside in rural areas where there is a significant lack of specialized workers in most sectors. The situation in Moldova has deteriorated still further since the full invasion of neighboring Ukraine, with an influx of refugees that are largely hosted at local community level, and the associated energy crisis, and spiraling inflation.
In many cases, there is a vicious cycle between health, risk factors for NCDs and low socio-economic status. NCDs strike persons when they should be their most productive, rendering some of them dependent on social benefits, while as the disease progresses, they become less able to work, more likely to face discrimination, isolation and other risk factors like depression, alcohol consumption. Every ninth inhabitant of the country lives in extreme poverty (absolute poverty rate 26.8% in 2022), especially the elderly in rural areas.
In consequence, life expectancy is decreasing (69.1 years), with disparities in rural area (68.5 years) comparing with urban area (69.8 years), as well as a difference of 8 years between women and man (73.1 years and 65.2 years) [NBS 2022]. Furthermore, primary disability in the working age population is increasing (10476 of new cases in 2022 compared with 9174 in 2020). More than 64% of this population are living in rural area [NBS 2022b]. With their multiple problems, these elderly persons have a high need for health and social care services, placing pressure on both the health and the social sector from a human resources and financial perspective, as well as being problematic from the aspect of availability in rural areas.
With their multiple problems, these elderly persons have a high need for health and social care services, placing pressure on both the health and the social sector from a human resources and financial perspective, as well as being problematic from the aspect of availability in rural areas.
Structural, social and political barriers and power imbalances in ensuring health equity
The insufficiency of programs for NCD prevention and management means that there is low adherence to treatment, despite that compensated drugs are covered by the national health insurance. This results in high incidence of acute episodes like heart attack and stroke that make demands of specialized assistance resulting in high costs of services, as well as out of pocket costs to the patients and their families.
The reasons for the challenges at local level are linked to the limited human resources, especially in coverage with family doctors/ general practitioners (on average 4.8 per 10 thousand population, in some districts 2.4) [NBS 2022a]. The cadre of the community nursing assistance was introduced in Moldova in 2014, to assist family doctors, and support with outreach and community work, but the number of them is limited (just 278 CN out of 597 full time positions in 2020 according to MoH) and the proper role of this position is not perceived especially in prevention and supporting vulnerable groups of population [NHIH 2022].
Given the close links between poor health and social-economic status, people living with NCDs are often more likely to contact social services in search of benefits or financial support. Community social workers (CSWs) (1162 CSWs in 2022 according to NSAA, at least one in each mayoralty) support the application for funds but were generally linking the person to the health services. Conversely, those that rather present to a family doctor are not cross-referred to access social services.
Interestingly, the concept of vulnerability in the social welfare sector in Moldova does not include NCD as a risk situation and is resulting in less attention to adult patients or elderly living in a family environment. Only in crises or cases of severe vulnerability (e.g. very bad life conditions, abuse, violence, high level of dependency and lack of care within the family, relatives, community or this person is in the role of carer (children, disabled or old person)), can a case management process be opened. Although, prevention of social vulnerability is recognised as a component of social protection, individual family and community resilience and wellbeing is only partially being approached mostly in child protection area, but also depending very much on the availability and capacity of personnel, particularly the first line representatives like CSW.
Although national regulatory frameworks were updated in the recent past towards improved multi-sectorial collaboration and to reduce social vulnerability, in reality integrated work modalities in working with vulnerable adults and elderly at rayon and community levels are still limited.
Interestingly, the concept of vulnerability in the social welfare sector in Moldova does not include NCD as a risk situation and is resulting in less attention to adult patients or elderly living in a family environment.
Shared responsibility for improving health and the wellbeing of population
The SDC “Healthy Life Project” works with the Ministry of Health and Ministry of Labour and Social Protection as well as the Local Public Authorities to promote an “Integrated People Centred Health Services (IPCHS)” approach to the management of NCDs and complex health and social needs.
The key intervention is to organise an inter-sectoral response to NCDs, whereby primary health care and community social workers jointly assess needs and also involve all relevant community actors and civil society, like education, police, civil society including specialised NGOs providing homecare, and volunteers, formal and informal caregivers and empowering the leading role of local public authorities.
The SDC “Healthy Life Project” works with the Ministry of Health and Ministry of Labour and Social Protection as well as the Local Public Authorities to promote an “Integrated People Centred Health Services (IPCHS)” approach to the management of NCDs and complex health and social needs.
Implementing IPCHS puts people in the middle of a services network and requires service providers to assess people’s needs and to coordinate their input accordingly. This includes the joint medico-social needs assessments of NCD patients and application of the case management for those with complex needs.
The community teams prepared through a capacity building process containing few stages of sectorial and multisectoral trainings aiming to strengthen the practical abilities of community medical assistants, understanding and application of the same definition for the wellbeing and sharing criteria of vulnerability, learning building blocks of integrated care as well as better know the reciprocal roles and responsibilities of different sectors.
These teams are supported to develop integrated care action plans based on locally available data and additional assessments to identify health and social vulnerability amongst patients with NCDs. Although action plans varied between districts, all interventions included awareness raising sessions, messages for primary and secondary prevention, reducing risk factors and adjusting lifestyle factors.General well-being indicators and people’s concerns were monitored, high risk patients identified and interventions for those with complex needs initiated.
These teams are supported to develop integrated care action plans based on locally available data and additional assessments to identify health and social vulnerability amongst patients with NCDs.
Results of implementation
A common monitoring and data collection instrument was developed and included also in the draft Regulation on Integrated Community Care proposed as a temporary solution to be approved by the District Councils before its approval through Governmental Decision that is at the second reading stage. These data collection was applied for all pilot communities and districts. The implementation of the integrated care action plans is monitored and analysed quarterly by the Raional Public Health Councils.
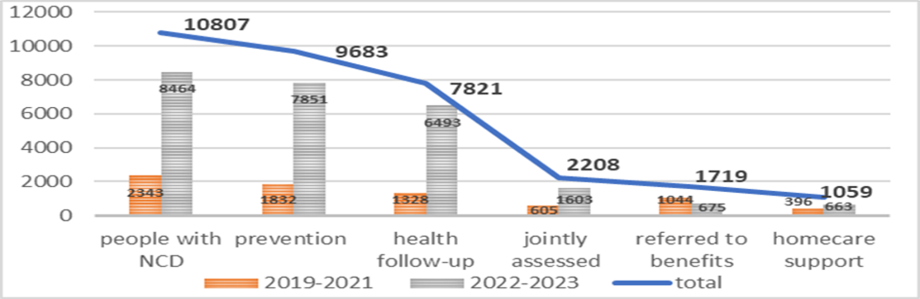
During the period of 2019-2023 years, integrated community care was applied in 40 communities of 20 pilot districts. A total of 10807 persons with NCD that are at the evidence at the family doctor were covered with different interventions, including with preventive activities (89.5%), health follow-up (72.3%), support in poverty (15.9%) and long-term care services (9.7%).
Fig.1 People with NCDs assisted in 2019-2023
By the end of 2024 year integrated community care will cover all 35 country districts and two municipalities and will increase to 74 pilot communities.
The Healthy Life project supports the implementation of integrated care approaches through improving quality of services, capacity building at the level of care, particularly related to Community Medical Assistance (CMA), social services and local public authorities. It promotes better inter-sectoral coordination of interventions, the use of common tools and procedures (case management for NCD patients, inter-sectorial needs assessment, geriatric assessment and setting up “one-stop-shops” such as community medico-social centres).
A reduction of acute cases and emergency calls, while keeping people in their own houses and communities are appreciated by decision-makers in the country and cherished by people with NCDs and their families. Moldova is also striving for integration to reduce the costs of specialized services, with less hospitalizations and to grasp these opportunities at community level, and this is timely as part of its wider EU succession planning process.
A reduction of acute cases and emergency calls, while keeping people in their own houses and communities are appreciated by decision-makers in the country and cherished by people with NCDs and their families.
Tatiana
Dnestrean is an integrated care and social assistance expert with extensive
work experience in the Moldovan Public System (Ministry of Labour and Social
Protection), Donor Projects (DFID, UNDP, USAID, UNICEF) and NGOs. Since 2018 she
works with the SDC Healthy Life Project on policy development and
conceptualisation of Integrated Community Care in NCD and strengthening
community nursing. Email
Ala Curteanu is a Moldovan Medical Doctor with a specialisation in paediatrics and a public health expert with more than 25 years’ experience working in the health sector in Moldova. Since 2017 Ala Curteanu holds the position of team leader of the SDC Healthy Life: Reducing the Burden of Non-Communicable Diseases Project Facilitation Unit, implemented by the Swiss Tropical and Public Health Institute in the Republic of Moldova. Email
Octavian
Pascaru is a general practitioner with a Masters in Public Health who works in
the SDC Healthy Life project to reduce the burden of NCDs. He has over 20 years
of work experience in the primary health care system, inclusively on palliative
care and has worked with UNHCR Moldova, the National Health Insurance Company
and several NGOs. Email
Helen
Prytherch PhD, MPH is head of the systems strengthening and health promotion
unit at the Swiss Tropical and Public Health Institute. Since 2018 she directs
the SDC Healthy Life Project, working closely with the local team in Chisinau.
Helen Prytherch also serves on the Board of Medicus Mundi Schweiz. Email
Konkrete Ansätze zur Bekämpfung gesundheitlicher Chancenungleichheit