For a long time, infectious diseases have been the dominating issue regarding the health of sub-Saharan African populations. Improved life health conditions, urbanization, economic development, changes in lifestyle are all contributing to a long-term shift in the burden of diseases toward an increase importance of non-communicable diseases (NCDs). If this trend is well recognized, health systems are much slower to adapt, and prevention of causes associated with NCDs remains largely neglected. This is particular the case of tobacco consumption, which sometime is not even mentioned in discussions about NCDs in Africa.
Lesezeit 8 min.
Photo by Bongani Ngcobo on Unsplash
The shifting picture of NCDs in Africa
Between 1990 and 2017, the total burden of disease (based on disability-adjusted life-years or DALYs) attributable to NCD rose from 18,6% to 29,8%, which represent a 67% increase in all-age total DALYs. Although most of this increase can be explained by population growth and ageing, the age-standardised DALY rate (per 100 000 population) due to NCDs in 2017 was almost equivalent to that of communicable, maternal, neonatal, and nutritional diseases. Cardiovascular diseases were the second leading cause of NCD burden in 2017 (151% of the total NCD burden), after the group of disorders categorised as other NCDs (191%). These categories were followed by neoplasms, mental disorders, and digestive diseases.
Although crude DALY rates for all NCDs have decreased slightly across sub-Saharan Africa, age-standardised rates are on the rise in some countries (particularly those in southern sub-Saharan Africa) and for some NCDs (such as diabetes and some cancers, including breast and prostate cancer). Tracheal, bronchus, and lung cancer increased over the period by 76.2% and Chronic obstructive pulmonary disease (COPD) increased by 60.5%. Research indicates growing burdens of diabetes, chronic respiratory diseases, chronic kidney disease, cardiovascular diseases, cancers, and mental and substance use disorders, in numerous countries in sub-Saharan Africa. Furthermore, sub-Saharan Africa is expected to see one of the largest increases in mortality due to NCDs globally. NCD risk factor surveillance in sub-Saharan Africa over the past decade indicates that most adults are exposed to at least one risk factor for NCDs, including tobacco consumption, harmful alcohol use, unhealthy diet, physical inactivity, obesity, or high blood pressure (Gouda, Hebe N., et al. 2019)
The NCD impact on lower income countries is often underestimated, despite the fact that 85% of premature deaths (between ages 30–69) from NCDs occur in low- and middle-income countries, making them a huge health and socioeconomic burden. NCDs – including heart disease, diabetes, cancer and respiratory disease – currently cause 7 out of every 10 deaths around the world. A new WHO report shows that close to 7 million deaths could be prevented by 2030 if low- and lower-middle-income countries were to make an additional investment of less than a dollar per person per year in the prevention and treatment of noncommunicable diseases (NCDs). Investing 1 dollar per person per year could save 7 million lives in low- and lower-middle-income countries (WHO 2021).
A new WHO report shows that close to 7 million deaths could be prevented by 2030 if low- and lower-middle-income countries were to make an additional investment of less than a dollar per person per year in the prevention and treatment of noncommunicable diseases (NCDs).
Africa is the continent where smoking has been increasing the most in the last 30 years. Among both males and females, the increase was of 104,1% in north Africa and the Middle East and of 74,6% in sub-Saharan Africa (Reitsma, Marissa B. et al., 2021). If we consider only the “potential” market for cigarettes in a country like Nigeria, where urban population are getting richer and lifestyle is changing fast, the perspective is chilling.
Especially the risk of initiation among young people and adolescent should be taken into account. In a study about age at smoking initiation and prevalence of cigarette use among 13 to 15 years old youths in sub-Saharan Africa, data from 9 countries was considered. Weighted prevalence of ever cigarette use ranged from 5.4% in Tanzania to 36.4% in Seychelles. Current cigarette use ranged from 1.0% in Tanzania to 15.4% in Seychelles. Susceptibility to smoking initiation ranged from 7.3% in Tanzania to 28.9% in Sierra Leone. In all countries, cigarette smoking prevalence was greater among male youths compared with female youths (e.g. in Gabon: 40.8% of male youths had ever smoked vs 17.1% of female youths). Among ever smokers, more than 20% of youths started smoking by age 8 years in Tanzania, Ghana, and Sierra Leone. In all study countries, more than 75% of youths who smoked initiated smoking before age 15 years (Chido-Amajuoyi, Onyema Greg, et al., 2021)
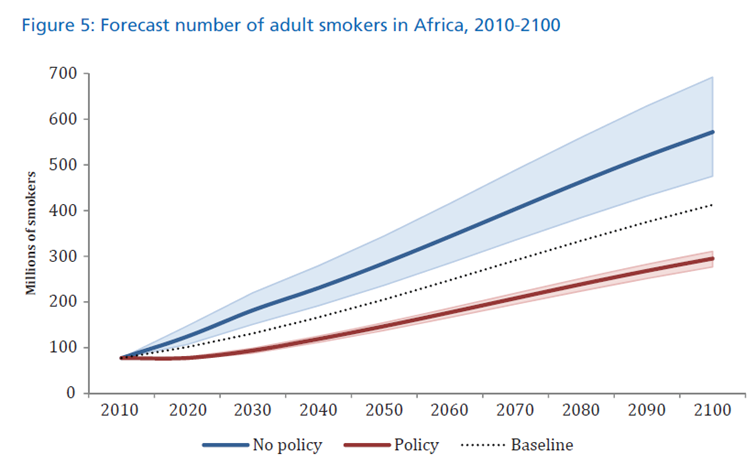
In 2013, about 77 million African adults smoked. If the tobacco industry is allowed to operate largely unregulated, this is expected to increase more than 7 times over to 572 million within the century. This evolution will depend very much on the prevention policies that will be adopted in African countries. In the absence of any effective policies, numbers will increase dramatically (Blecher, Evan, et al., 2013).
Source: Blecher, Evan; Ross, Hana (2013): Tobacco Use in Africa: Tobacco Control through Prevention. American Cancer Society.
From smoking to NCDs: a slow progression
The impact of smoking on health can need a long period of time to fully unfold. The smoking epidemic has been modelled in stages, and in this respect sub-Saharan Africa is still largely considered at sub-epidemic levels, even if the situation is changing at an increasing pace (Thun, Michael, et al. 2012).
Africa is very often talked about as if it was a unity, while in reality it is a complex patchwork of countries, languages and cultures, which gives to the first continent where humans appeared a unique and rich diversity. This diversity reflects itself in many fields, including health and consumption behaviours, and particularly so in tobacco consumption. If tobacco arrived very early on the African west coast, brought there by the Portuguese slave traders, its adoption was not uniform all over the continent. The results are that Africa has one of the lowest prevalence rates with only 14% of the overall adult population smoking, which is low compared the America with 23% or the Eastern Mediterranean region with 31%.
If some African countries are among the highest smokers, like Mauritania, where adults consume 41 cigarettes every day makes them the biggest world smokers of all, or Tunisia, Libya and Egypt, some other countries are among the lowest, like Nigeria, Ghana, and Ethiopia. The problem is not only limited to traditional cigarettes, for instance in Mauritania over 18% of 13-15 years students reported currently using electronic cigarettes in 2018 (GYTS, 2018). Trends also differs greatly, and Mozambique saw an increase of 220% in cigarette consumption over the past 16 years. Difference can be explained partly by cultural differences. In Tunisia, tobacco appears to be a social accepted norm, with 58% of the population being a declared smoker. On the opposite side, Nigeria where the prevalence is only of 6%, smoking seems to be restricted to a certain social standing (SEATCA).
Photo by Dimitri Bong on Unsplash
The need to a radical change in NCD prevention in global health: where is tobacco prevention?
How much the fight against tobacco has been integrated in global health strategies?
In the SDC Health Policy, NCD prevention is mentioned, and tobacco as a risk factor is also mentioned, but only once. Is this enough to translate words into effective actions? Tobacco prevention should be included like a transversal condition in all health-related projects, like environmental aspects are nowadays. Supporting hospital activities in a specific country should come under the condition to make the supported hospital completely smoke-free.
We tried to identify if in the network of MMS, any organization specifically integrating the fight against tobacco as a clear and explicit element of their strategies. We might have missed some information, but we where unable to identify any organization that did so. We also know that some member organisations of MMS accepted in the past money from big tobacco industries. Is this ethically acceptable? Should MMS adopt a guideline requiring all its members to better integrate NCD prevention in their activities and to clearly reject all money coming from tobacco industries?
MMS has been already vocal in the past about the incompatibility of the interests of the tobacco industry and the global health engagement of Switzerland (MMS 2019). Our country cannot pretend to defend the “interests” of some “Swiss” companies like the big tobacco industries and seriously engage in global health. Big tobacco companies only care about their billion-dollar profit (they are located in Switzerland only because of fiscal advantages) and they could not care less about global health, nor about health in Switzerland.
MMS has been already vocal in the past about the incompatibility of the interests of the tobacco industry and the global health engagement of Switzerland. Our country cannot pretend to defend the “interests” of some “Swiss” companies like the big tobacco industries and seriously engage in global health.
Photo by Random Institute on Unsplash
Lobby and advertisement: the Marlboro Man now lives in Africa
Some countries where prevalence is low and where economic development opens new potential huge markets, are the perfect prey for the tobacco industry that has for a long time concentrated its marketing and lobby activities in richer countries. A perfect example of this is Nigeria, which ratified the FCTC but where implementation of national tobacco control law has been slow (Egbe, Catherine O. et al., 2019). In countries like Nigeria, the industry has been particularly active to aggressively advertise to kids. Schools and playgrounds are surrounded by advertising for Marlboro or Lucy Strike. It is also common that single sticks are sold because those are more affordable to kids. The result is that in a number of countries in Africa, children and youth use tobacco twice as much as their parents because the industry has successfully managed to attract children through advertising, sponsorship and promotion (Boseley S. et al., 2018). In Nigeria, 5.6 percent of adults (age 15+) use tobacco products, but among youth (ages 13-15), 15.4 percent use tobacco products (boys 19.2 percent and girls 11.1 percent) (Tobacco-Free Kids).
In countries like Nigeria, the industry has been particularly active to aggressively advertise to kids. Schools and playgrounds are surrounded by advertising for Marlboro or Lucy Strike.
Fortunately, initiatives to fight against the spreading of the tobacco epidemic are arising, and not only from public health officials. The Nigerian National Film Video & Censors Board (NFVCB) has announced new plans to pass a non-smoking law in Nollywood movies. Adedayo Thomas made the revelation during an entertainment industry stakeholders roundtable in Lagos in December 2021, stressing that "The tobacco industry uses a sophisticated marketing mix to promote smoking on set and in the entertainment sector" and that “Entertainment stakeholders are deliberately targeted by the tobacco industry either through financial inducement, misinformation, and other subtle approaches to further glamorize smoking in the entertainment sector" (pulse.ng 2021).
African represents a huge market with one of the greatest possibilities to increase their market shares for the tobacco industry. Their new “scramble to Africa”, i.e. their fight to conquer this deadly market is already on. What will we do to prevent this from happening?
References
Blecher, Evan; Ross, Hana (2013): Tobacco Use in Africa: Tobacco Control
through Prevention. American Cancer Society.; Méndez, David;
Alshanqeety, Omar; Warner, Kenneth E. (2013): The potential impact of
smoking control policies on future global smoking trends. In Tob Control
22 (1), pp. 46–51. DOI: 10.1136/tobaccocontrol-2011-050147.
Chido-Amajuoyi, Onyema Greg; Fueta, Patrick; Mantey, Dale (2021): Age at
Smoking Initiation and Prevalence of Cigarette Use Among Youths in
Sub-Saharan Africa, 2014-2017. In JAMA Netw Open 4 (5), e218060. DOI: 10.1001/jamanetworkopen.2021.8060. https://jamanetwork.com/journals/jamanetworkopen/f...
Egbe, Catherine O.; Bialous, Stella A.; Glantz, Stanton (2019):
Framework Convention on Tobacco Control Implementation in Nigeria:
Lessons for Low- and Middle-Income Countries. In Nicotine & tobacco research : official journal of the Society for Research on Nicotine and Tobacco 21
(8), pp. 1122–1130. DOI: 10.1093/ntr/nty069. And Siddiqi, Kamran
(2019): Tobacco Use in Sub-Saharan Africa: The Risks and Challenges. In Nicotine & tobacco research : official journal of the Society for Research on Nicotine and Tobacco 21 (8), pp. 999–1000. DOI: 10.1093/ntr/ntz086. https://watermark.silverchair.com/nty069.pdf?token...
Gouda, Hebe N.; Charlson, Fiona; Sorsdahl, Katherine; Ahmadzada, Sanam; Ferrari, Alize J.; Erskine, Holly et al. (2019): Burden of non-communicable diseases in sub-Saharan Africa, 1990–2017: results from the Global Burden of Disease Study 2017. In The Lancet Global Health 7 (10), e1375-e1387. DOI: 10.1016/S2214-109X(19)30374-2. https://www.thelancet.com/pdfs/journals/langlo/PII...
Reitsma, Marissa B.; Kendrick, Parkes J.; Ababneh, Emad; Abbafati,
Cristiana; Abbasi-Kangevari, Mohsen; Abdoli, Amir et al. (2021):
Spatial, temporal, and demographic patterns in prevalence of smoking
tobacco use and attributable disease burden in 204 countries and
territories, 1990–2019: a systematic analysis from the Global Burden of
Disease Study 2019. In The Lancet. DOI: 10.1016/S0140-6736(21)01169-7. https://www.thelancet.com/action/showPdf?pii=S0140...
Thun, Michael; Peto, Richard; Boreham, Jillian; Lopez, Alan D. (2012):
Stages of the cigarette epidemic on entering its second century. In Tob Control 21 (2), pp. 96–101. DOI: 10.1136/tobaccocontrol-2011-050294. https://tobaccocontrol.bmj.com/content/21/2/96
Luciano Ruggia is the executive director of the Swiss
association for tobacco control (AT Switzerland) and a board member of
Medicus Mundi Switzerland. Email
Teilen
Bleiben Sie informiert – abonnieren Sie unseren Newsletter.