Piggybacking on maternal and neonatal health programs to address NTDs
Von Bharath Kumar Sundar
How can nations prioritize addressing diseases that in many cases affect less than 1 in 10’000 people, especially in low resource settings? The neglected tropical diseases (NTD) roadmap 2030 emphasizes applying integrated approaches, to further accelerate elimination goals. In Nepal, one such a NTD program implemented in the Lumbini province, by the government of Nepal, supported by FAIRMED, a Swiss NGO, is piggybacking on the flagship maternal and child health program, to address NTDs, specifically, Leprosy and Lymphatic filariasis.
More than a billion people across the world, 1 in every 6, are infected by at least one of the twenty Neglected Tropical Diseases (NTDs). Many of them are ancient diseases, have a burden at least the same as tuberculosis and malaria, yet remain largely overlooked, best characterized as a “chronic pandemic”. Most NTDs have low mortality rates but people suffering are subject to severe lifelong disabilities. The ‘neglect’ of NTDs is therefore not only of the diseases but the people too, who represent the bottom billion, the poorest of the poor, most marginalized, stigmatized and often with no political voice. The systematic neglect is well represented in the official development assistance provided to NTDs, a mere 0.6% share compared to 36.3% for HIV. The NTD roadmap 2030 from the World Health Organization (WHO) identifies two main cross-cutting approaches to tackling their burden, ‘mainstreaming into health systems’ and ‘coordination with relevant programs’.
Project Setting
The Essential Health Project (EHP) is a registered health project partnering with the Nepal government, managed by the Swiss NGO, FAIRMED, along with other civil society organizations, tackling a wider scope of health systems strengthening, with focused activities in both MNH and NTD (focus on Leprosy & Lymphatic Filariasis) programs. The focus on these two NTDs, stems from the high co-endemicity, very similar self-care management methodologies and functioning joint services in Nepal by various NGOs in partnership with local government. The geographical spread of the EHP project is in three districts in the Terai plains of Southern Nepal, namely Kapilvastu, Rupandehi and Nawalparasi West. The EHP has been running since 2019 with the goal of improving the health status of communities through accountable and equitable health service delivery systems. As of 2021, the project has reached 8918 pregnant mothers and new-born, 573 NTDs (Leprosy + Lymphatic Filariasis) affected persons, trained 825 health workers, 1728 female community health volunteers (FCHVs) and 326 health mother groups (HMGs) which have 4865 members.
More than a billion people across the world, 1 in every 6, are infected by at least one of the twenty Neglected Tropical Diseases (NTDs). Many of them are ancient diseases, have a burden at least the same as tuberculosis and malaria, yet remain largely overlooked, best characterized as a “chronic pandemic”.
Piggybacking on community level MNH program and structures
Rationale: One program that has made significant progress driven by sustained investments in recent years in Nepal, is maternal and neonatal health (MNH), with maternal mortality rates dropping by close to 70% since 2000. Three key activities that have driven progress in Nepal with MNH are strengthening of primary health care centers, establishment of community directed interventions and sustained knowledge diffusion through mothers’ groups. There is growing evidence in how NTDs disproportionately affect women and children in Nepal. Not only during pregnancy due to anemia and iron deficiency but over the life-course for socio-cultural reasons and the stigma it causes. Therefore, identifying pathways through which MNH programs and engaging women can lead to effective interventions tackling NTDs, is critical.
Health leadership: Municipal, District and Provincial health departments
Community members: Leprosy & Lymphatic filariasis Self-Help-Groups (SHGs) and local civil society organizations (CSOs)
There is growing evidence in how NTDs disproportionately affect women and children in Nepal. Not only during pregnancy due to anemia and iron deficiency but over the life-course for socio-cultural reasons and the stigma it causes.
FCHV: Female Community Health Volunteers – Community level maternal & child health program. The cadre was created to enable safe birthing and motherhood. They are members living in the local community they work in.
Health Mother Groups: A group of usually 15-20 women of childbearing age, in each small village, formed specifically to disseminate government programs and MNH related best practices. One of them is elected to be the FCHV. These mother groups are formed by the local government in partnership with the community members, and form a critical part of the MNH structures in the community.
Health post in-charge: They are not medical doctors, but health assistants whose responsibility it is to ensure the smooth functioning of that ward’s health post and is directly responsible for execution of the maternal and child programs. The responsibility also includes managing ANM, AHW, Skilled birth attendant (SBA) and a sanitation worker.
AuxiliaryNurseMidwife: Responsible for antenatal, birthing, and postnatal care of women attending the birthing center located withing the health post.
AuxiliaryHealthWorker: Responsible for outpatient department, monthly outreach clinics and skin camp coordination.
SelfHelpGroup: Group of people affected by either leprosy or lymphatic filariasis. They are officially registered, meet once a month, are trained on self-care by health post in-charge and registered in the health post to facilitate timely follow-ups if needed.
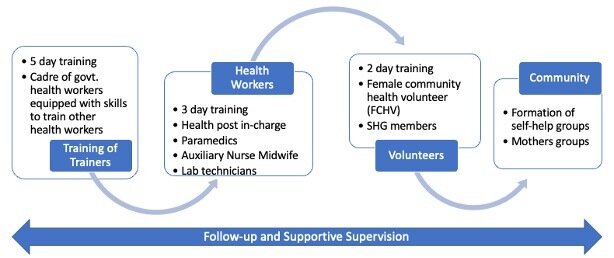
The starting point of this integration is naturally the MCH programs and structures. It starts with first creating a pool of NTD trainers, through a training of trainers. This is a 5-day training and involves doctors who are government health workers from the region and based in the region. This is then cascaded down to the health workers who are based in the periphery health posts, the first point of service delivery to the people in the community. This is 3-day training that involves practical real-life scenarios on when to screen, suspect, diagnose and confirm NTDs, for example, during ANC visits, or immunization camps or monthly outreach camps or post-natal care (PNC) home visits etc. This is often provided to health post in-charges, nurse midwives and auxiliary health workers. They then train community health volunteers and persons affected. This way the system is strengthened on NTD knowledge and practical implementation in everyday work of the health system.
Figure-1: The training cascade that is the trigger for integration
Key modes of how the intersection happens
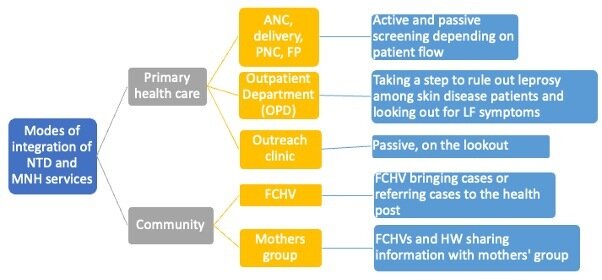
Community Awareness: Trained community health volunteers (FCHV) disseminate NTD awareness messages through the mothers’ groups meetings and their community visits. The mothers then become key channels through which awareness further spreads within the community.
Case detection: The FCHVs also play a key role in various other health campaigns (immunization, Vitamin A, NCD camps) and are visiting door to door most of the community members within their catchment areas. Opportunistic screening and initial suspicion of leprosy or lymphatic filariasis is done through this.
Another point of intersection is during the ANC visits from pregnant women to their local health post. This is when the NTD-trained nurse midwives, who conduct the ANC check-ups, also screen the women for NTDs endemic in that region. Once someone has been diagnosed positive for an NTD, say leprosy, they are counseled and recommended for treatment. Where challenges do remain is in following-up with further contact tracing in the communities. This is a complex issue owing to the highly stigmatized nature of some of these NTDs, where maintaining privacy becomes extremely critical. The ANC visit compliance rate is increasing consistently in Nepal and has been significantly incentivized monetarily by national and local governments. This provides a major boost and rationale for this integration.
Yet another intersection happens from the NTD-trained auxiliary health worker, visits the community once a month, during outreach camps. These usually happen in communities that live more than an hour’s walk away from the nearest health post. During these outreach clinics the AHW screens for leprosy and lymphatic filariasis amongst those who visit these monthly camps. Once suspected, they are referred to the health post for further confirmatory processes. Here is another point where frequent loss to follow-up have been addressed by ensuring the community health volunteers then reach out to the concerned community members to visit the health post and seek service, usually along with social mobilizers of the EHP project.
Community based rehabilitation: Those identified with disabilities or physical impacts from the NTDs already manifesting, are provided with self-care training by the trained health workers and FCHVs. This ensures effective wound care management and improvement of conditions. The affected persons are also at a certain frequency provided with supportive supervision on self-care by trained health workers and social mobilizers in the community, often in their homes.
Figure-2: Flow-chart of the modes of integration of MNH and NTD
The engine that coordinates and manages these complex partnerships and engagement is the project managers and social mobilizers, who are members of the local villages, recruited into the project by FAIRMED and its partner Nepalese civil society organizations. They ensure consistent coordination at all three tiers of the federal structure of Nepal and persistent, rigorous mobilization at a household-by-household level in the community, with the people.
What is coming up - Sustainability and country ownership
The key next steps are for the scaling up to all endemic districts within Nepal, within the country national program and limited external dependency. An operational research study has recently been concluded on this piggybacking approach, on what works, what doesn’t and where the challenges lie. The publishing of this research in the coming months will provide key insights.
Two key actions in the recent months indicate optimism for such developments:
The first one being this NTD training cascade started in the EHP project, adapted, and updated, and launched as the government of Nepal (Lumbini Province) official NTD training manual.
The second one is for the first time, backing this training manual up with governmental budgetary allocation towards its implementation in the most recent June 2022 budget cycle.
These are green shoots that if nurtured, sustained, and followed up could lead to a big boost towards addressing the needs of people affected by NTDs in Nepal.
Recent visit by Swiss Alliance against NTDs (SANTD) and International Federation of Anti-Leprosy Associations (ILEP) delegates
Alongside the 2022 international NGO conference on NTDs in Kathmandu, a 3-person delegation from ILEP and SANTD, visited the EHP project in Lumbini Province, to see this integration between MNH and NTDs in action. This will pave way for wider international dissemination of such pragmatic operational and opportunistic integration mechanisms to address the persistent and often nationally, severely under-funded NTD programs.
Bharath Kumar Sundar works as program officer in Bern, for the Swiss NGO, FAIRMED. His work covers Nepal and Sri Lanka, addressing public health topics in highly vulnerable populations. The scope of his work in Nepal and Sri Lanka is in strengthening local primary health care systems, with special focus on neglected tropical diseases (NTDs). Email